The Mediterranean Child Cohort Network (CHILDREN_FIRST) was created in early 2022. CHILDREN_FIRST is a Mediterranean network of a multi-country child cohort infrastructure that will focus its resources and activities on the longitudinal assessment of key environmental (non-genetic) risk factors in association with the temporal evolution of respiratory, cardiometabolic or neurodevelopmental outcomes in primary school children populations in five Mediterranean countries (Cyprus, Greece, Spain, Albania and Israel). The vision of the CHILDREN_FIRST network is to establish a world-class research infrastructure specializing in the development and application of personalized medicine/prevention models towards improved disease prevention and prediction in children. The mission of the CHILDREN_FIRST network is to design and apply research of the highest quality standards, education, advocacy and outreach protocols and activities towards improved disease prevention and prediction models; this will be achieved using the principles of personalized prevention and the suite of exposomic tools to characterize the environmental determinants of temporal disease process dynamics for the children of the Mediterranean region, and beyond.
The overall theme of the CHILDREN_FIRST network is based upon the personalized prevention approach and the exposome concept applications in children’s health. Personalized medicine or personalized prevention models study differences in children’s genes, environments and lifestyles, hence, they can provide knowledge about enhanced risk profiling and population stratification, but also about how such information can be used to improve children’s health (1). The exposome concept was proposed in an attempt to elucidate the role of the environment in the development of chronic diseases (2), since it was shown that environmental factors contribute about 80-90% of the risk for some chronic diseases (3). To our best knowledge, CHILDREN_FIRST is the first globally comprehensive personalized prevention program for primary school aged children in the Mediterranean region, based on exposome methodologies and tools to generate important biomarkers of exposure/effect and also be able to better predict and prevent disease in this susceptible critical lifetime window.
Rationale
Mediterranean region is considered a hot spot for climate change, as it is hit hard by rising air temperatures, wildfires, droughts, reduction in air quality, and adverse weather events, all of which are projected to increase in frequency in future years (4). Forecasts for the Mediterranean region show that the mean temperature is expected to rise by about 1–3°C in the next three decades and between 3.5–7 °C by the end of the 21st century, ranking the region ahead of projected global temperature changes (4).
In the last decade 2009-2019, the five most common causes of death in Cyprus, Greece, Italy, Albania and other Mediterranean (Med) countries remain almost the same, and these are: cardiovascular disease (i.e., coronary heart disease and stroke), diabetes, cancer and chronic obstructive pulmonary disease (5). Obesity is a major risk factor for several NCDs, including cardiovascular disease, diabetes and some cancers3 and childhood obesity rates have increased globally (6). Particularly in the Mediterranean countries (Cyprus, Greece, Italy, Spain), overweight prevalence rates in children are the highest in Europe (42-43%) (7). Data from the International Incidence of Childhood Cancer suggest that Mediterranean countries carry some of the highest world age-standardized cancer incidence rates for the ages 0-19 years old (8).
Children exhibit increased susceptibility to environmental exposures because of their rapid development, differences in behaviors and metabolism and their parents’ environmental exposures (9). Based on the predicted obesity prevalence rates among 2-year-old children from the CHOICES simulation model, a steep increase of obesity prevalence was estimated for their primary school years (5-11 years old), indicating that this period is a critical window of susceptibility (10).
Moreover, three out of six identified lung function risk trajectories, which were associated with childhood factors i.e. asthma, bronchitis, pneumonia, allergic rhinitis, eczema, contributed to 75% of chronic obstructive pulmonary disease cases and their impact was aggravated by adult factors (11). Preventing both early adverse exposures in children groups with varying risks of susceptibility to NCD risk factors is of utmost importance to EU (Fig. 1).
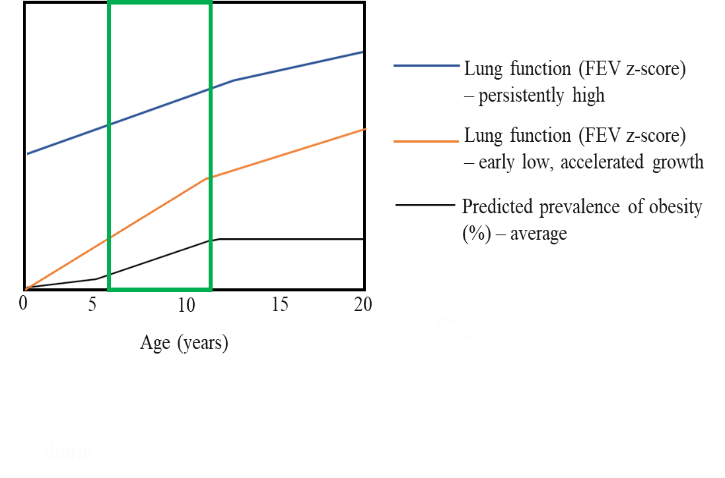 Figure 1 Indicative prevalence of obesity (black line) and lung function trajectories (blue and yellow) from birth to 20 years old. The primary school age group that is shown within the green frame. The figure shows 1) the critical window of susceptibility for children aged 6-11 years old and 2) the differential expression of lung function risk, depending on various risk factors and the importance of personalized prevention for children (10,11).
Figure 1 Indicative prevalence of obesity (black line) and lung function trajectories (blue and yellow) from birth to 20 years old. The primary school age group that is shown within the green frame. The figure shows 1) the critical window of susceptibility for children aged 6-11 years old and 2) the differential expression of lung function risk, depending on various risk factors and the importance of personalized prevention for children (10,11).
References:
1.European Commission. Personalised Medicine. Published 2020. https://research-and-innovation.ec.europa.eu/research-area/health/personalised-medicine_en
2.Haddad N, Andrianou XD, Makris KC. A Scoping Review on the Characteristics of Human Exposome Studies. Curr Pollut Rep. 2019;5(4):378-393. doi:10.1007/s40726-019-00130-7
3.Willett WC. Balancing Life-Style and Genomics Research for Disease Prevention. Science. 2002;296(5568):695-698. doi:10.1126/science.1071055
4.Lelieveld J, Hadjinicolaou P, Kostopoulou E, et al. Climate change and impacts in the Eastern Mediterranean and the Middle East. Clim Change. 2012;114(3):667-687. doi:10.1007/s10584-012-0418-4
5.Murray CJL, Aravkin AY, Zheng P, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020;396(10258):1223-1249. doi:10.1016/S0140-6736(20)30752-2
6.de Onis M, Blössner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92(5):1257-1264. doi:10.3945/ajcn.2010.29786
7.World Health Organization Regional Office for Europe. Childhood Obesity Surveillance Initiative. Highlights 2015-2017.; 2018. https://www.euro.who.int/__data/assets/pdf_file/0006/372426/WH14_COSI_factsheets_v2.pdf
8.Steliarova-Foucher E, Colombet M, Ries LAG, Hesseling P, Moreno F, Shin HY, Stiller CA,. International Incidence of Childhood Cancer, Volume III (Electronic Version). International Agency for Research on Cancer; 2017. https://iicc.iarc.fr/results/comparative-tables/00-all-neoplasms.pdf
9.Vrijheid M, Casas M, Gascon M, Valvi D, Nieuwenhuijsen M. Environmental pollutants and child health—A review of recent concerns. Int J Hyg Environ Health. 2016;219(4-5):331-342. doi:10.1016/j.ijheh.2016.05.001
10.Ward ZJ, Long MW, Resch SC, Giles CM, Cradock AL, Gortmaker SL. Simulation of Growth Trajectories of Childhood Obesity into Adulthood. N Engl J Med. 2017;377(22):2145-2153. doi:10.1056/NEJMoa1703860
11.Bui DS, Lodge CJ, Burgess JA, et al. Childhood predictors of lung function trajectories and future COPD risk: a prospective cohort study from the first to the sixth decade of life. Lancet Respir Med. 2018;6(7):535-544. doi:10.1016/S2213-2600(18)30100-0












 Wednesday, 06 December, 2023
Wednesday, 06 December, 2023